홈 > 연구소 > 논문 / 학술활동
연구소
마마파파&베이비의 핵심인 베이비 드림 난임 연구소는
그간의 연구학술 성과에 안주하지 않고,
늘 한계를 뛰어넘기 위해 노력합니다.
인공수정시술을 하기 전 얼마나 오래 금욕을 해야 하는가?
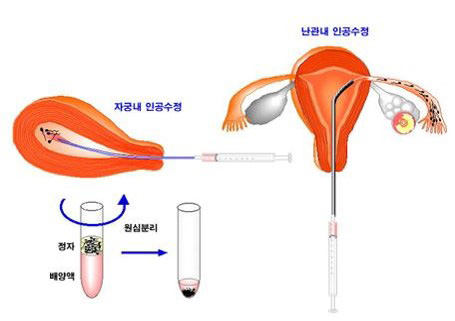
2016년 유럽불임학회(ESHRE) P-062 How long should we keep ejaculatory abstinence (EA) before intrauterine insemination (IUI)? (인공수정시술을 하기 전 얼마나 오래 금욕을 해야 하는가?)
J.W. Kim, K.H. Lee, I.H. Park, H.G. Sun, H.J. Chi, S.G. Kim, Y.Y. Kim, S.J. Kwak, J.Y. Park, C.S. Yoo
Mamapapa & Baby Obstetrics & Gynecology Clinic, Infertility, Ulsan, South Korea.
Study question
Is ejaculatory abstinence before IUI essential factor for pregnancy?
Summary answer
The period of ejaculatory abstinence before IUI is not related with pregnancy rates
What is known already
The total number of motile sperm inseminated has been cited as the most predictive index of conception in IUI cycles. Intercourse on the day of hCG administration might cause concern about a lower recovery of total motile sperm. However, optimal period of ejaculatory abstinence before IUI is not yet established.
Study design, size, duration
Retrospective analysis of 804 IUI cycles performed between April and December in 2015. The period of ejaculatory abstinence before IUI, semen analysis parameters of the ejaculate (pre-wash) and the insemination specimen (post-wash) for IUI, and pregnancy rate following ovulation induction and IUI were recorded.
Participants/materials, setting, methods
The whole ejaculate was prepared for insemination using a technique of density gradient separation with centrifugation. Ejaculatory period before IUI was divided into 3groups (0-2 days, 3-5days, >5 days).
Main results and the role of chance
In each group, age, semen volume, sperm motility (pre-wash) and liquefaction time did not show significant differences. Although the longer EA period, the more total motile sperm count (pre-wash) was observed (88.2, 137.2, 194.7(*106/ml), p<0.05), but there were no significant differences in post-wash total motile sperm count (8.3, 10.9, 11.7 (*106/ml), p>0.05). Total pregnancy rate was 19.4% (144/804). There were no significant differences among three groups in the pregnancy rate (22.5% (14/80), 18.7% (53/310), 19.3% (77/414); p>0.05).
Limitations, reasons for caution
To identify the period of EA, we asked for questionnaire survey to patients. So, there could be recall bias. Prospective randomized studies with larger sample size will be required to confirm our conclusions.
Wider implications of the findings
There were few studies about relation between pregnancy rate and period of EA before IUI. Our result shows that period of EA before IUI does not affect pregnancy rate. Therefore, we can advise that abstinence before IUI and the interval of intercourse seldom affect pregnancy outcome.
-
 2017년 유럽불임학회(ESHRE) P-
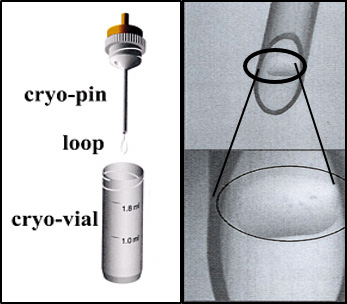
Cryo-loop와 Hemi-straw를 이용한 인간 배아 유리화 동결에서 해동 후 손상되지 않은 배아와 임상 결과의 비교.
2017년 유럽불임학회(ESHRE) P-
Cryo-loop와 Hemi-straw를 이용한 인간 배아 유리화 동결에서 해동 후 손상되지 않은 배아와 임상 결과의 비교.
-
 2016년 미국불임학회(ASRM) P-595
반복착상 실패 환자 에서 면역치료요법이 유용할 것인가; 특히 높은 자연살해세포를 가진 환자에서?
2016년 미국불임학회(ASRM) P-595
반복착상 실패 환자 에서 면역치료요법이 유용할 것인가; 특히 높은 자연살해세포를 가진 환자에서?
-
 2016년 미국불임학회(ASRM) P-555
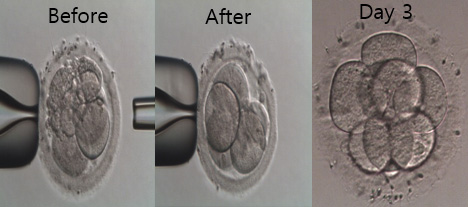
2일 째 파편화된 인간 배아에서 파편제거는 순차적 배아의 발달과 임상적 결과를 유의하게 증가시킨다.
2016년 미국불임학회(ASRM) P-555
2일 째 파편화된 인간 배아에서 파편제거는 순차적 배아의 발달과 임상적 결과를 유의하게 증가시킨다.
-
 2016년 미국불임학회(ASRM) P-317
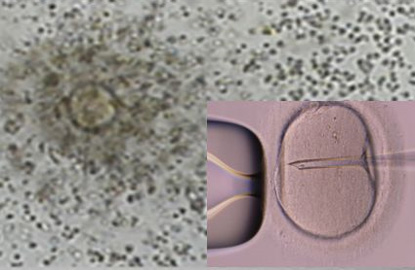
정자 DNA 파편화 지수가 높은 환자에서 ICSI가 전통적인 IVF에 비해 임신율을 유의하게 증가시켰다.
2016년 미국불임학회(ASRM) P-317
정자 DNA 파편화 지수가 높은 환자에서 ICSI가 전통적인 IVF에 비해 임신율을 유의하게 증가시켰다.
-
 2016년 미국불임학회(ASRM) P-263
연속 배아 채점 시스템은 Time-lapse 모니터링 시스템 대신 사용할 수 있습니다.
2016년 미국불임학회(ASRM) P-263
연속 배아 채점 시스템은 Time-lapse 모니터링 시스템 대신 사용할 수 있습니다.
-
 2016년 유럽불임학회(ESHRE) P-021
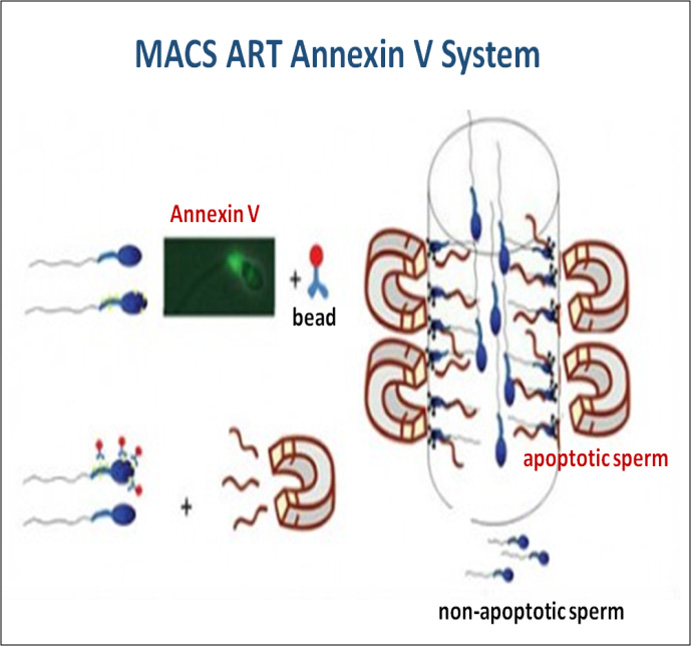
중층원심분리와 자석활성화세포분리 방법의 병용은 정액샘플의 정자 DNA손상지수를 유의하게 감소시킨다.
2016년 유럽불임학회(ESHRE) P-021
중층원심분리와 자석활성화세포분리 방법의 병용은 정액샘플의 정자 DNA손상지수를 유의하게 감소시킨다.
-
 2016년 유럽불임학회(ESHRE) P-022
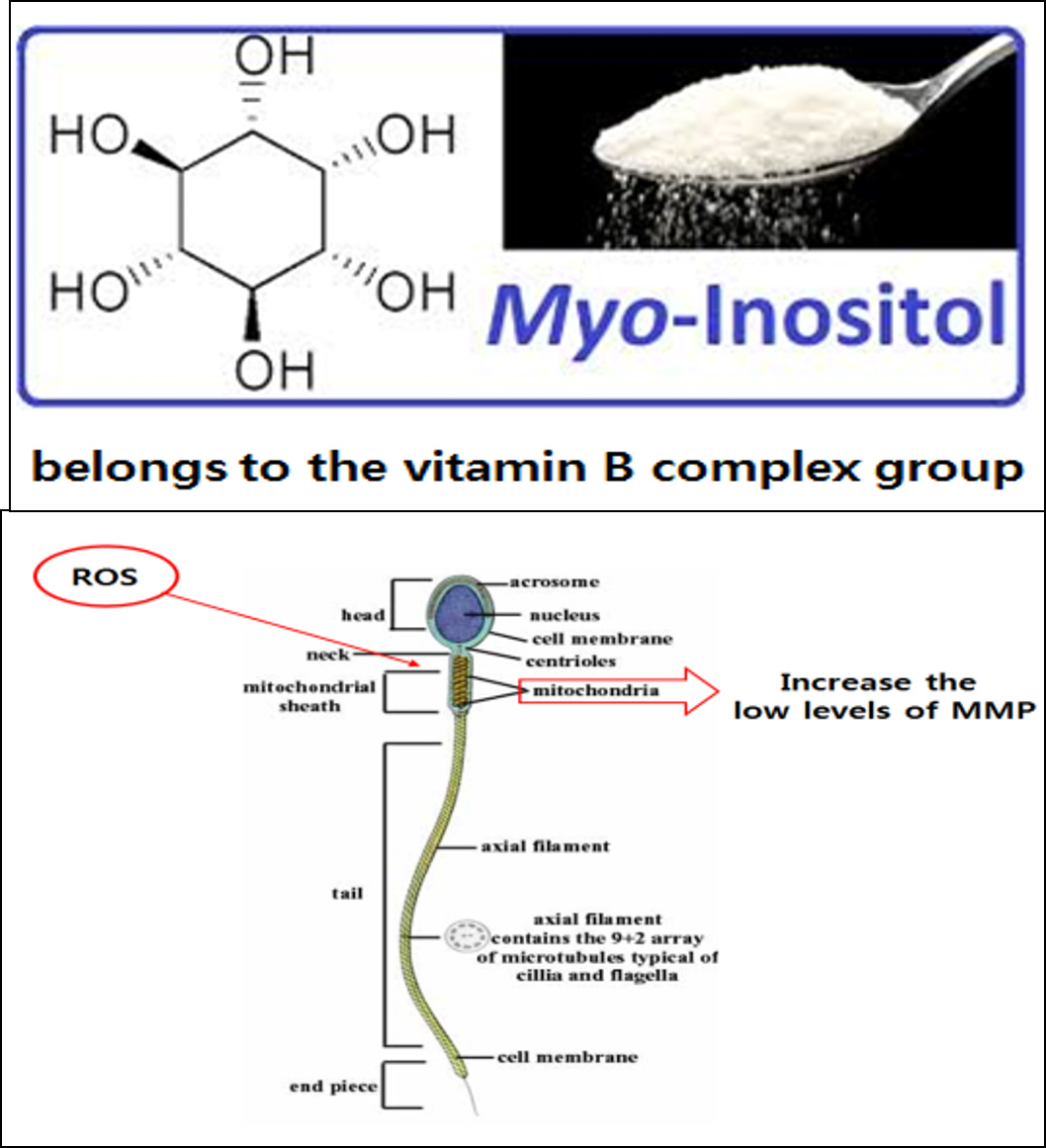
정액처리 배양액에 Myoinositol의 첨가는 무력정자증 환자의 인공수정시술 시 정자의 운동성과 임신율을 향상시켰다.
2016년 유럽불임학회(ESHRE) P-022
정액처리 배양액에 Myoinositol의 첨가는 무력정자증 환자의 인공수정시술 시 정자의 운동성과 임신율을 향상시켰다.
-
 2016년 유럽불임학회(ESHRE) P-182
다낭성난소증후군 환자의 동결융해배아 이식을 위한 효율적이고 환자친화적인 자궁내막 준비방법; letrozole을 이용한 배란유도
2016년 유럽불임학회(ESHRE) P-182
다낭성난소증후군 환자의 동결융해배아 이식을 위한 효율적이고 환자친화적인 자궁내막 준비방법; letrozole을 이용한 배란유도
울산광역시 남구 삼산로 247 마마파파앤베이비 빌딩 15F - 17F
TEL 052-258-6006 / FAX 052-258-6026
Copyright © mamapapa&baby All Rights Reserved.