홈 > 연구소 > 논문 / 학술활동
연구소
마마파파&베이비의 핵심인 베이비 드림 난임 연구소는
그간의 연구학술 성과에 안주하지 않고,
늘 한계를 뛰어넘기 위해 노력합니다.
과배란 시험관 시술에서 임신실패 시 동결란 이식 준비까지 회복기간이 필요한가?
2012년 유럽불임학회 (ESHRE) P-317 Whether recovery period after failed COH-IVF cycle is required in the subsequent FET cycle? (과배란 시험관 시술에서 임신실패 시 동결란 이식 준비까지 회복기간이 필요한가?)
S.G. Kim1, K.H. Lee1, I.H. Park1, H.G. Sun1, J.H. Lee1, Y.Y. Kim1, E.M. Choi1.
1 Mamapapa&baby Obstetrics Gynecology Clinic, Infertility Lab., Ulsan city, Korea South.
INTRODUCTION
While COH (controlled ovarian hyperstimulation) is commonly used to recruit multiple follicles for cycles of IVF, it alters the endometrial development and can impair the endometrial receptivity. COH cycle may also influence adverse effect inpregnancy of the subsequent FET (frozen-thawed embryo transfer) cycle. The purpose of this study is to verify whether recovery period after failed COH-IVF cycle can affect pregnancy rate of the subsequent FET cycle.
MATERIALS AND METHODS
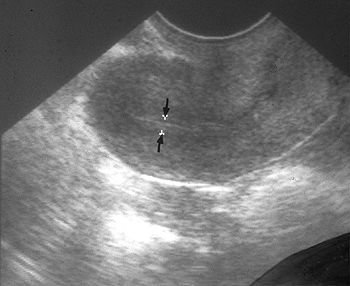
518 cycles from patients who underwent frozen thawed embryo transfer from September 2009 to December 2011, were analyzed. The patients were divided into two groups as follows. In group 1, 174 patients immediately started endometrial preparation on the 3rd day of the first menstrual cycle after failed IVF-ET cycle. Patients of group 2 (344) waited at least one resting cycle before starting endometrial preparation. Cryopreserved embryos were transferred to patients either in natural cycleor in a hormonally manipulated artificial cycle following preparation of the endometrium with estradiol and progesterone. Embryos were frozen on day 3 using a vitrification protocol. Pregnancy identified through detection of G-sac in transvaginal ultrasound examination. Outcomes were statistically analyzed by t test. P value <0.05 was considered statistically significant.
RESULTS
During the study period the 518 FET performed and resulted in 177 pregnancies (34.2%). There was no difference between both groups in patient age (34.0±4.4 in group 1 and 34.6±4.0 years in group 2) and endometrial thickness (9.2 ±2.0 and 9.8 ±2.0 mm). Embryo survival to freezing-thawing (78.9±20.5% and 80.7±20.0%), the number of embryos transferred per patient (2.2±0.4 and 2.2±0.4) and embryo quality were also comparable in both groups. However, the pregnancy rate was significantly higher in group 2 (37.8%) than group 1 (27.0%, p=0.018).
CONCLUSION
The study reveals that starting endometrial preparation for FET at the first menses, immediately after the stimulated cycle, does impair the pregnancy rate. Probably, it may be due to impaired endometrial receptivity by alterations of the endometrial development after previous COH-IVF cycle. Therefore, in order to achieve an increase of pregnancy rate in FET, recovery period is needed for one or more months after a failed COH-IVF cycle.
-
 2013년 미국불임학회(ASRM) P-1052
인공수정시술에서 정자 처리 과정에서 빛을 차단하는 것의 효과
2013년 미국불임학회(ASRM) P-1052
인공수정시술에서 정자 처리 과정에서 빛을 차단하는 것의 효과
-
 2013년 미국불임학회(ASRM) P-1040
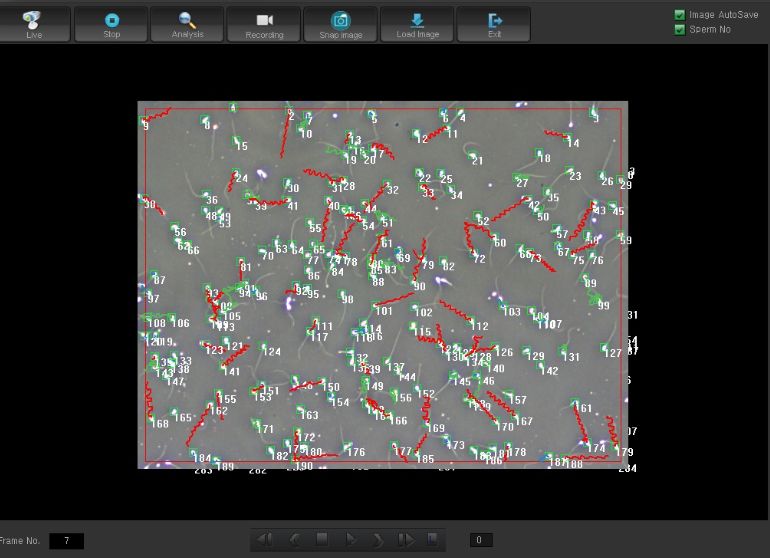
시험관 시술에서 임신 예측을 위하여 운동성 있는 총 정자 숫자의 효용성
2013년 미국불임학회(ASRM) P-1040
시험관 시술에서 임신 예측을 위하여 운동성 있는 총 정자 숫자의 효용성
-
 2013년 미국불임학회(ASRM) P-398
AMH≥3ng/ml인 경우 시험관 시술에서 시작 용량은 112.5IU로 하여도 성공적인 임신에 충분하다.
2013년 미국불임학회(ASRM) P-398
AMH≥3ng/ml인 경우 시험관 시술에서 시작 용량은 112.5IU로 하여도 성공적인 임신에 충분하다.
-
 2013년 미국불임학회(ASRM) P- 303
성숙 난자가 3개 이하인 경우 미세수정을 시행하는 것이 반드시 필요한가?
2013년 미국불임학회(ASRM) P- 303
성숙 난자가 3개 이하인 경우 미세수정을 시행하는 것이 반드시 필요한가?
-
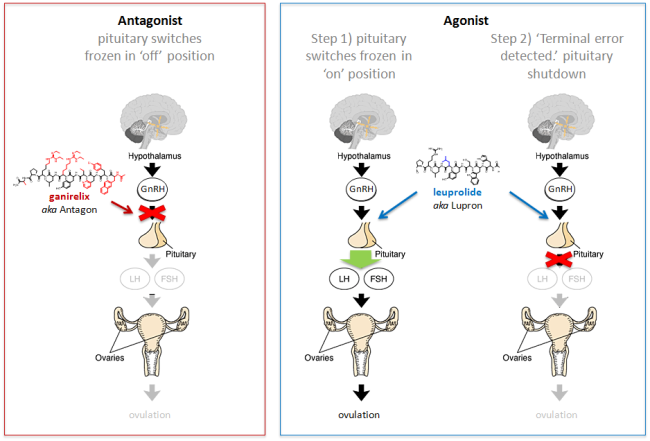 2013년 미국불임학회(ASRM) P-121
동결란 이식에서 GnRH 길항제 요법과 효능제 요법이 수정란의 상태에 어떠한 영향을 미치는가?
2013년 미국불임학회(ASRM) P-121
동결란 이식에서 GnRH 길항제 요법과 효능제 요법이 수정란의 상태에 어떠한 영향을 미치는가?
-
 2012년 유럽불임학회 (ESHRE) P-317
과배란 시험관 시술에서 임신실패 시 동결란 이식 준비까지 회복기간이 필요한가?
2012년 유럽불임학회 (ESHRE) P-317
과배란 시험관 시술에서 임신실패 시 동결란 이식 준비까지 회복기간이 필요한가?
-
 2012년 유럽불임학회 (ESHRE) P-200
3일째 동결란 이식하는 경우 늦게 분열하는 수정란과 8세포의 수정란 사이에 임신능력의 차이는 유사하다.
2012년 유럽불임학회 (ESHRE) P-200
3일째 동결란 이식하는 경우 늦게 분열하는 수정란과 8세포의 수정란 사이에 임신능력의 차이는 유사하다.
-
 2012년 미국불임학회 (ASRM) P-51
동결란 이식에서 자궁내막의 두께의 중요성 : 호르몬 보충법과 자연주기 동결란 이식법 사이에서 차이점
2012년 미국불임학회 (ASRM) P-51
동결란 이식에서 자궁내막의 두께의 중요성 : 호르몬 보충법과 자연주기 동결란 이식법 사이에서 차이점
울산광역시 남구 삼산로 247 마마파파앤베이비 빌딩 15F - 17F
TEL 052-258-6006 / FAX 052-258-6026
Copyright © mamapapa&baby All Rights Reserved.