홈 > 연구소 > 논문 / 학술활동
연구소
마마파파&베이비의 핵심인 베이비 드림 난임 연구소는
그간의 연구학술 성과에 안주하지 않고,
늘 한계를 뛰어넘기 위해 노력합니다.
AMH≥3ng/ml인 경우 시험관 시술에서 시작 용량은 112.5IU로 하여도 성공적인 임신에 충분하다.

2013년 미국불임학회(ASRM) P-398 The 112.5IU r-hFSH starting dose is enough for successful IVF in AMH≥3ng/ml. (AMH≥3ng/ml인 경우 시험관 시술에서 시작 용량은 112.5IU로 하여도 성공적인 임신에 충분하다.)
SeokGi kim1, JiHye Lee1, Il Hae Park1, Hong Gil Sun1 and Kyeong Ho Lee1.
1Infertility Lab., Mamapapa&baby obstetrics and Gynecology, HWASHIN BLD 4F 1367-5 DAL-DONG, NAM-KU ULSAN, x, Republic of Korea, 680-805
OBJECTIVE
Controlled ovarian hyperstimulation(COH) is needed in order to improve the pregnancy rate in IVF cycles. Recently, there has been an interest in using a much lower dosage of follicle stimulating hormone(FSH)for mild stimulation in IVF protocols. The purpose of this study was to assess the mild stimulation with starting dose of recombinant human FSH(r-hFSH) 112.5IU could be enough for successful IVF outcomes in patients with AMH ≥3ng/ml in IVF cycles.
DESIGN
Retrospective study
MATERIALS AND METHODS
We retrospectively reviewed657 consecutive cycles of 594normo-ovulatroywomen(AMH ≥3ng/ml) who underwent IVF-ET treatment over a 3-year period (2010 -2012) at our institution.
Our study population was divided into two groups according to r-hFSH starting dose for COH-IVF cycles. Group A: r-hFSH(Gonal-Fⓡ) starting dose 112.5IU (n=257), Group B: r-hFSH starting dose 150IU (n=400) in women with AMH ≥3ng/ml. Outcomes were compared the number of oocytes retrieved, total dose of r-hFSH used, total number of r-hFSH stimulation days, clinical pregnancy and abortion rate between the two groups.
RESULTS
The total dose of r-hFSH administered was significantly different between the group A and the group B(1055.1 IU and 1365.5 IU, respectively, p<0.01). The total number of r-hFSH administration days (9.6days (5?17) and 9.1days (9?16), p=0.08).mean number of transferred embryo(2.0±0.2 and 2.0±0.2, p=0.263), the mean endometrial thickness (10.9±6.5 and 10.4±6.1 mm, p=0.07) and embryo quality were comparable in both groups. Although the number of retrieved oocytes (14.9 ± 6.8 vs. 13.3 ± 6.1 respectively; P<0.01) and fertilized oocytes(9.1 ± 4.9 vs. 8.8 ± 4.3 respectively; P=0.02) were significantly higher in group A than group B. However, the clinical pregnancy rate (63.4% vs58.3%, p=0.139)and abortion rate (12.9% vs13.3%) were not significantly different between both groups.
CONCLUSION
In our results,a total mean r-hFSH dose of 1055.1IU with the 112.5IU starting dose in COH cycle was sufficient for the number of retrieved oocytes and the pregnancy rates in patients with AMH≥3ng/ml.Therefore, These seemsclear that a subset of patients with AMH ≥3ng/ml undergoing ovarian stimulationcan be adequately treated with a 112.5 IU starting dose ofr-hFSH.
-
 2013년 미국불임학회(ASRM) P-1052
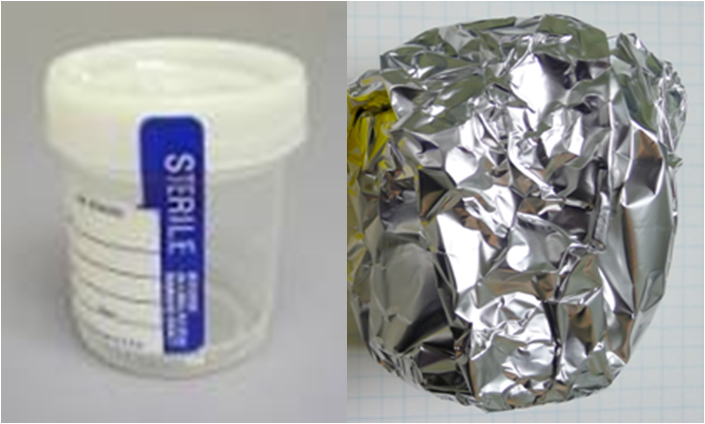
인공수정시술에서 정자 처리 과정에서 빛을 차단하는 것의 효과
2013년 미국불임학회(ASRM) P-1052
인공수정시술에서 정자 처리 과정에서 빛을 차단하는 것의 효과
-
 2013년 미국불임학회(ASRM) P-1040
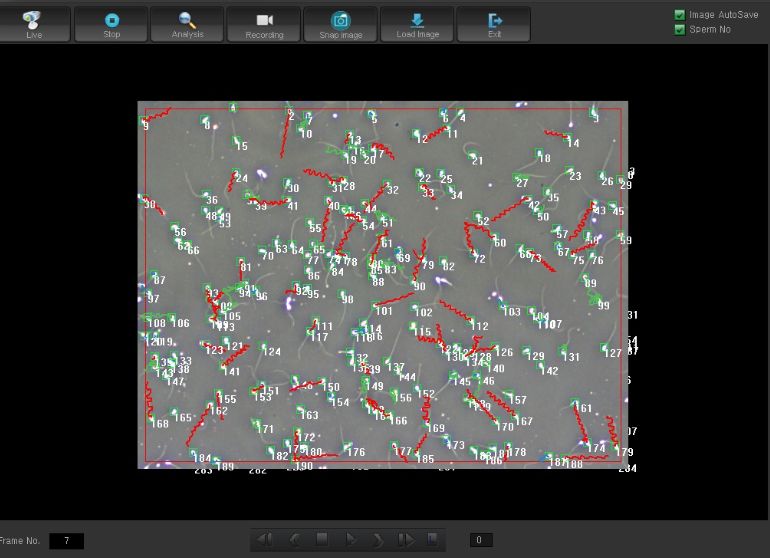
시험관 시술에서 임신 예측을 위하여 운동성 있는 총 정자 숫자의 효용성
2013년 미국불임학회(ASRM) P-1040
시험관 시술에서 임신 예측을 위하여 운동성 있는 총 정자 숫자의 효용성
-
 2013년 미국불임학회(ASRM) P-398
AMH≥3ng/ml인 경우 시험관 시술에서 시작 용량은 112.5IU로 하여도 성공적인 임신에 충분하다.
2013년 미국불임학회(ASRM) P-398
AMH≥3ng/ml인 경우 시험관 시술에서 시작 용량은 112.5IU로 하여도 성공적인 임신에 충분하다.
-
 2013년 미국불임학회(ASRM) P- 303
성숙 난자가 3개 이하인 경우 미세수정을 시행하는 것이 반드시 필요한가?
2013년 미국불임학회(ASRM) P- 303
성숙 난자가 3개 이하인 경우 미세수정을 시행하는 것이 반드시 필요한가?
-
 2013년 미국불임학회(ASRM) P-121
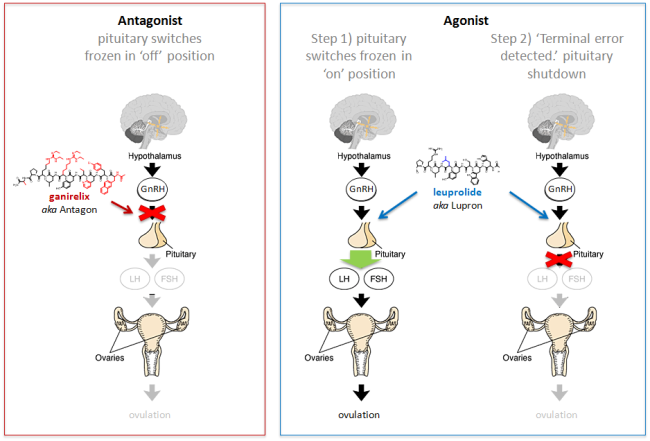
동결란 이식에서 GnRH 길항제 요법과 효능제 요법이 수정란의 상태에 어떠한 영향을 미치는가?
2013년 미국불임학회(ASRM) P-121
동결란 이식에서 GnRH 길항제 요법과 효능제 요법이 수정란의 상태에 어떠한 영향을 미치는가?
-
 2012년 유럽불임학회 (ESHRE) P-317
과배란 시험관 시술에서 임신실패 시 동결란 이식 준비까지 회복기간이 필요한가?
2012년 유럽불임학회 (ESHRE) P-317
과배란 시험관 시술에서 임신실패 시 동결란 이식 준비까지 회복기간이 필요한가?
-
 2012년 유럽불임학회 (ESHRE) P-200
3일째 동결란 이식하는 경우 늦게 분열하는 수정란과 8세포의 수정란 사이에 임신능력의 차이는 유사하다.
2012년 유럽불임학회 (ESHRE) P-200
3일째 동결란 이식하는 경우 늦게 분열하는 수정란과 8세포의 수정란 사이에 임신능력의 차이는 유사하다.
-
 2012년 미국불임학회 (ASRM) P-51
동결란 이식에서 자궁내막의 두께의 중요성 : 호르몬 보충법과 자연주기 동결란 이식법 사이에서 차이점
2012년 미국불임학회 (ASRM) P-51
동결란 이식에서 자궁내막의 두께의 중요성 : 호르몬 보충법과 자연주기 동결란 이식법 사이에서 차이점
울산광역시 남구 삼산로 247 마마파파앤베이비 빌딩 15F - 17F
TEL 052-258-6006 / FAX 052-258-6026
Copyright © mamapapa&baby All Rights Reserved.